
Episode 8.02 Frailty Scores
Presented by: Dr Iain Wilkinson & Dr Jo Preston
Core Faculty: Sarah Jane Ryan, Dr Dan Thomas
Guest input: Dr Richard Dodds – many thanks for the advice and guidance
Release date – August 13th 2019
Learning Objectives
Knowledge
- To understand the advantages of frailty scoring
Skills
- To recognise when frailty scoring might be beneficial
Attitudes
- To appreciate that the intent of frailty scoring is to tailor care to prevent harms
- To see frailty identification as an opportunity to tailor care
Show Notes
Definition
Frailty is a distinct clinical entity from normal ageing (but related to ageing) consisting of multi-system dysregulation leading to a loss of physiological reserve, resulting in a state of increased vulnerability to stressors and therefore potential harms.
Two main theories
- Fried: Phenotype
- Rockwood: Accumulation of Deficits
Main Discussion
Discuss difference between frailty scoring high risk groups vs screening as a principle.
Benefits of identifying frailty
Frailty Scoring aims to identify those who may be at high risk of living with frailty and benefit of interventions to reduce the risk of frailty related harms.
- Increased risk of falls
- Increased admissions to hospital
- Longer lengths of stay
- High risk of readmission
- Increased dependency with activities of daily living
- With likelihood to require some form of care
- Trajectory is towards institutional care (nursing home)
- Excess risk of death
Can we do anything about this?
Fried: Yes
- Improve physical function
- Improve nutrition
- Improve psychological status
Rockwood: Yes
- Ameliorate physical deficits
- Improve physiological reserve
- Treat medical conditions
Frailty – a fixed or dynamic state…?
Fried’s studies around phenotype showed that frailty is a dynamic process
> Reminder: fatigue, unintentional weight loss, low grip strength, slow walking speed
> Trajectory is towards more frail states in general terms.
- If pre-frail:
- Those scoring 1- more likely to become non-frail
- Those scoring 2- more likely to progress to frail
- If frail:
- Those scoring 3 have the best chance of becoming pre-frail
- Those scoring 4-5 more likely to progress to death
- Very rare to revert from frail to non-frail (0-0.9% chance)
This is important to consider because scoring aims to identify those who can benefit from intervention which can improve their overall wellbeing, health and function, rather than to simply code or quantify it. Scores based on fixed data points then may not be so helpful in identifying those for whom intervention is beneficial. This is where it sometimes can feel like ‘just another score’.
Fit For Frailty
- Advises against routine population screening: no evidence base, costly and ?acceptable
- But recommends trying to identify at risk groups e.g. at risk of admission / readmission / clinical groups of people however little evidence to support this at present. May highlight individuals with no reversibility which is less helpful, Parallel to sensitivity and specificity: a score may identify frailty well, but does it help identify those that will benefit most from it being identified?
- Provide training in frailty recognition to all staff
- When recognised must undertake some form of review e.g. CGA and mostly in primary care.
- Consider referral to Geriatric Medicine when complex, diagnostic uncertainty or challenging symptoms.
Fit For Frailty by the British Geriatrics Society 2014
Advises
- Looking for causes in functional decline
- Ensuring reversible conditions are considered and addressed
- Individualise care through drug reviews, using clinical judgement and personalised goals when applying disease based guidance.
- Generating personalised shared care and support plans including treatment goals, plans for urgent care and EOLC.
- Information shared between agencies.
- Developing local protocols and pathways for frailty.
Some Scores
Fried – covered already
- High focus on physical elements but recognises psychological
- Not readily used in clinical practice
- 3 states:: frail / pre-frail / non-frail so discrimiation is less than in some other scorings.
Frailty Index (Rockwood) – accumulation of deficits
- Good reproducibility and based on operationalising CGA domains
- Deficits may be symptoms, signs, disease states, specific functional deficits
- Cut off between fitness and frailty around 0.25
- Seems to be a threshold around 0.67, where any more leads to death
Benefits
- Appears to fit with theory of declining physiological reserve
- Idea of gradation of frailty rather than present or absent
- Clear association with increasing frailty index and worse outcomes
- Better predictor than actual age: Fit for age, frail for age
Drawbacks
- A large number of items needed- at least 30, so ? easy to apply
- Cut-offs may vary, at what point should we intervene?
Another which labels as frail or not frail is: Prisma-7 (≥3 = frail)
- Age >85
- Male sex
- Any health probs that require you to limit activities?
- Do you need help on a regular basis?
- Any health probs that require you to stay at home?
- In case of need can you count on someone close to you?
- Do you regularly use a mobility aid to get about?
Simple to use, can be self-administered. Helps to guide the interventions that may be required / need further assessment.
From the FI, two further scores have emerged: CFS and eFI.
Clinical Frailty Score
- Pictorial and physically focused although wording does mention ADLs
- Dementia mentioned but this is often hard to define as moderate or mild if don’t know the patient well or particularly familiar with dementia
- Therefore cognition, mood, social elements not included.
- 1 to 9: very fit to very frail and including palliative
- Good correlation to FI
- Easily implemented and followed with minimal need for training.
eFI – GP level data
- Autogenerated
- Common criticisms e.g. need to go to GP, dependent on recording.
- What to do with it when weren’t meaning to e.g. gets close to screening.
TGUG
- Stand up, walk 3 m, turn around, sit down again.
- Over 10 seconds is abnormal.
Walking speed
- Less than 0.8m/sec
- > 5secs to walk 4m
Of those over 75, 1 in 3 will have slow walking speed and score on one of these two – so clinical assessment needed to exclude monopathology. Could therefore use a two-stage approach but no evidence for this in general.
Prisma plus TGUG good sensitivity but only moderate specificity
Sens and spec based on prevalence so more frailty more accurate- eg outpatient, social services etc, therefore supports case finding approach.
Edmonton Frail Scale
- Multiple domains based around CGA: nutrition, medication use, cognition, mood, function (incorporates TGUG), social support, continence.
- Takes time to administer face to face: takes about 20 mins on average.
- Guides interventions
- 5 outcomes: not frail, vulnerable, mildly frail, moderately frail, severely frail.
Frailty VIG
VIG = Spanish Catalan abbreviation for CGA
22 questions assessing 25 deficits
“Prospective, observational, longitudinal study of geriatric patients followed for 24 months or until death. n = 590 admitted to an Acute Geriatric Unit in Barcelona. Administration time for the Frail-VIG index ranged from 5 to 10 min. good discriminative capacity for the degree of frailty and a high predictive capacity for mortality at 12 and 24 months. more research is needed to confirm the validity of this instrument in other populations and settings, the Frail-VIG may provide clinicians with a RGA method and also a reliable tool to assess frailty in routine practice.”
Domains included:
- Functional: iADLs like money and medication management, telephone use. ADLs
- Nutritional
- Cognitive Impairment
- Emotional: Depressive syndrome, insomnia / anxiety
- Social vulnerability
- Geriatric Syndromes: delirium, falls, pressure ulcers, polypharmacy, dysphagia
- Severe symptoms: pain, dyspnoea
- Diseases: by system
Hospital Frailty Risk Score
- Cluster analysis to identify a group of older people (≥75 years) admitted to hospital who had high resource use and diagnoses associated with frailty.
- Created a Hospital Frailty Risk Score based on ICD-10 codes that characterised this group.
- In separate cohorts, we tested how well the score predicted adverse outcomes and whether it identified similar groups as other frailty tools.
Benefit: provides hospitals and health systems with a low-cost, systematic way to screen for frailty and identify a group of patients who are at greater risk of adverse outcomes and for whom a frailty-attuned approach might be useful. Work being done at NHS England on this in special groups at present e.g. oncology, renal cohorts.
Non-physical frailty & Resilience
Social frailty:
- Social vulnerability only modestly correlated with frailty
- Higher in women and with advancing age
- Associated with excess mortality
Cognitive frailty e.g. dementia / high risk of delirium: CFS, VIG,
Depression and anxiety
- Frailty associated with adverse psychological wellbeing: Fried, Edmonton, VIG,
While some of the scores do address this, this is probably the gap between many of them and clinical practice. Nice article recently highlighting this and links to other types of reserve, or resilience….
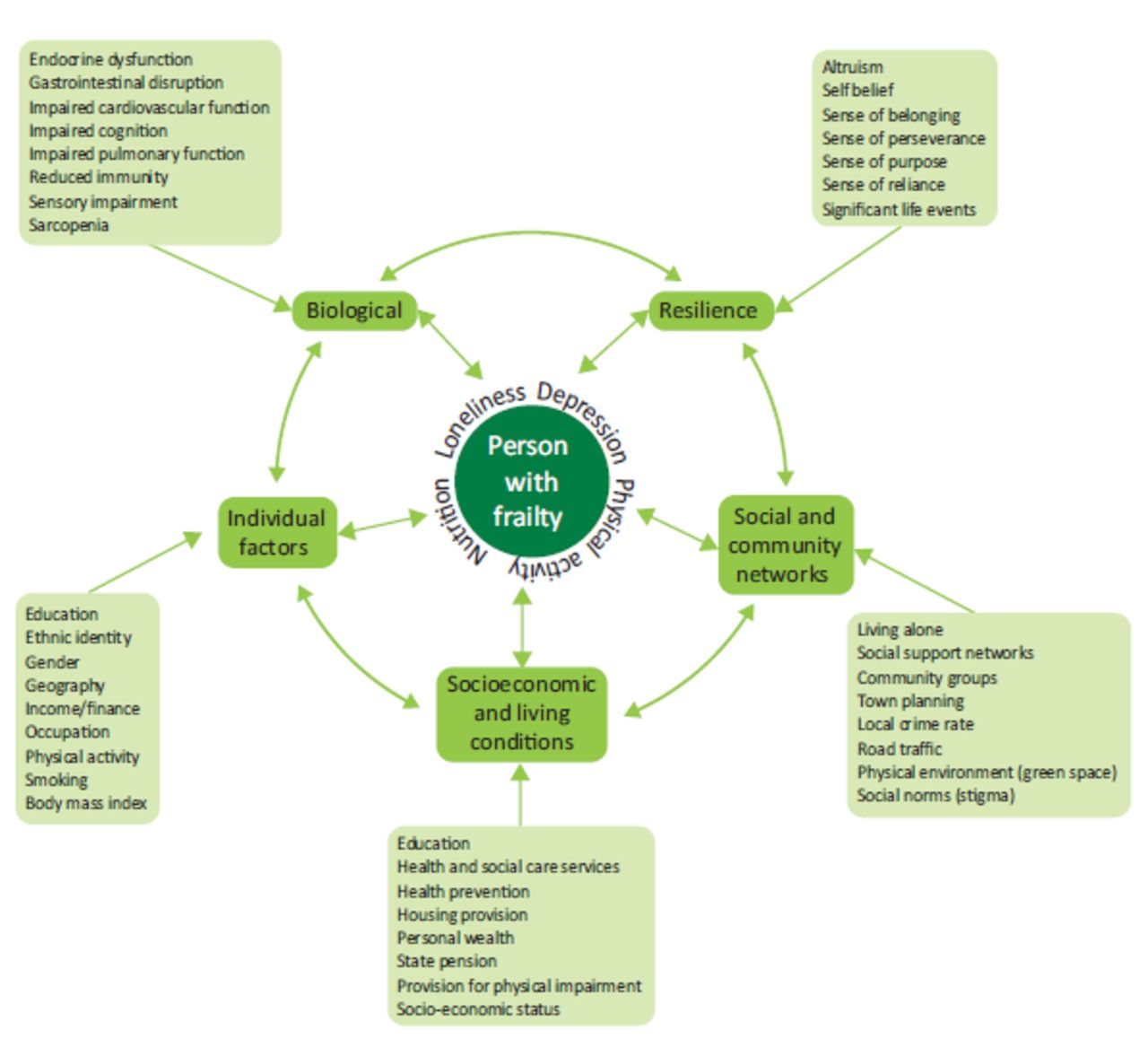
“Frailty is a common condition in later life in which minor stressors may result in major changes in health. While the biological mechanisms of frailty are increasingly understood, relationships with the wider determinants of health, health inequalities and the concept of resilience are less well-established and the role of the clinician in their modification is less well understood.
The wider determinants are the modifiable conditions in which people are born, grow, work and live, and the wider set of systems shaping the conditions of daily life. They interact across the life course, driving a well-recognised social gradient in health. The wider determinants are closely linked to the concept of resilience, which is the process of effectively negotiating, adapting to or managing significant sources of stress or trauma. Better recognition of the relationship between frailty, the wider determinants, inequalities and resilience can enable a framework around which policy responses may be developed to build resilience in people living with frailty at an individual and community level as well as enabling clinicians to better identify how they may support their patients.”
Frailty, Inequality and Resilience. Hale, Shah & Clegg. Clinical Medicine 2019
“We would like to suggest that properly addressing frailty within health systems will require no less than a complete reorientation of the health system away from a disease focus towards person-centred, coordinated and integrated care as advocated by the World Health Organisation and others.”
Curriculum Mapping
NHS Knowledge Skills Framework
- Core 2 Level 2
- Core 4 Level 1
- Core 5 Level 1
- HWB1 Level 2
- HWB2 Level 2
- HWB3 Level 1
- HWB4 Level 3
- HWB6 Level 2
- IK3 Level 1
Foundation Programme
- Section 1.4. Keeps practice up to date through learning and teaching – Self Directed Learning
- Section 3.10. Recognises, assesses and manages patients with long term conditions
- Section 10.5. Health promotion, patient education and public health
Core Medical Training
- The Patient as a central focus of care
- Managing long term conditions and promoting patient self- care
- Health promotion and public health
- Geriatric Medicine
- Musculoskeletal
GPVTS
- 3.01 Healthy People: promoting health and preventing disease
- 3.05 Care of Older Adults
- 3.20 Care of People with Musculoskeletal Problems
Geriatric Medicine Specialty Training
Principal Objectives:
- 1. Perform a comprehensive assessment of an older person, including mood and cognition, gait, nutrition and fitness for surgery in an in-patient, outpatient or community setting, including day hospitals
- 3. Diagnose and manage those with chronic disease, disability and frailty in an in-patient, out-patient, day hospital and community setting
Core Knowledge Objectives:
- 3.2.2 Common Geriatric Problems (Syndromes)
- 3.2.3 Presentations of Other Illnesses in Older Persons: Non-specific, weight loss, musculoskeletal
- 3.2.5 Rehabilitation in Older Persons: Different measures (assessment scales) used, Medical and social models of management of functional limitation.
- 3.2.9 Health Promotion
Core Curriculum Grids:
- 27. Comprehensive Geriatric Assessment
- 29. Diagnosis and Management of Chronic Disease and Disability
- 44. Care of Older People living with Frailty



