
Presented by:
Dr Iain Wilkinson (Consultant Geriatrician East Surrey Hospital)
Dr Jo Preston (Consultant Geriatrician St George’s Hospital)
Faculty:
Claire Gillespie, Nurse, Royal Sussex County Hospital
Dr Gabor Szekely, General Practitioner, Brighton
SJ Ryan, Physiotherapist, University of Brighton
Mary NÍ Lochlainn, Academic Clinical Fellow, Kings College Hospital London

Broadcast Date: 12th September 2017
CPD log
Click here to log your CPD online and receive a copy by email.
Tweetchat #MDTeaClub
We will be hosting a ‘journal club’ type tweet chat to discuss topics raised in the episode on 20th September at 8.30pm BST using #MDTeaClub
Join us to discuss topics raised in the episode. We will post a chat summary here after it has taken place in case you miss it.
Social Media spots this week
Geriatrics for Juniors:
Geriatrics for Juniors 2017 is here! Saturday 4th November in Newcastle. See https://t.co/AKnciymDip for full details & registration.
— AEME (@ElderlyMedEd) February 21, 2017
Show notes:
See PDF format
- Learning Outcomes:
- Knowledge:
- To understand the changes associated with ageing which may impact on their sexual life
- To recall how common it is for older adults to have active sex lives
Skills:
- To be able to approach conversations regarding sexuality
- To assess sexual expression, including in the context of cognitive impairment
Attitudes:
- To see sexual needs and expression as a normal part of life course regardless of age.
- To consider the sexual needs as part of holistic assessment.
Definitions:
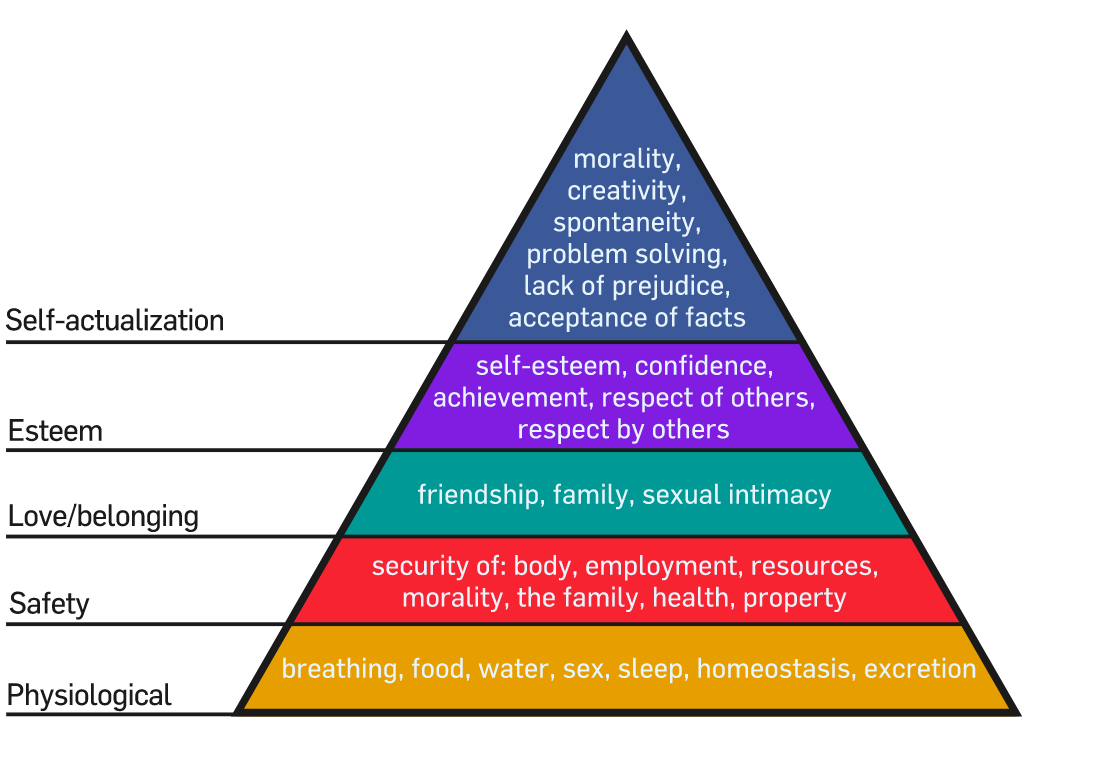
Rather than defining sex (there are websites that can help you with this. We’ll instead define how sex fits into normal adult life – Maslow’s hierarchy of needs
{kind=link}
In this episode we will discuss the factors that influence the maintenance of this in later life.
In a large survey carried out by AARP the group (1670 adults over 45y.o.) tried to define what a happy sexual relationship looks like. Those who were the most satisfied tended to have:
- – A sexual partner (not necessarily a spouse)
- – Frequent sexual intercourse (more than once a week but not necessarily daily)
- – Good health (self and partner)
- – Low levels of stress
- – Absence of financial worries
In this
Sex, Romance and Relationships: 2009 AARP Survey of Midlife and Older Adults
Key points from discussion
Sexual desire in Older Age.
Wellbeing
AARP survey found:
- – 28% report having sexual intercourse once a week or more on average in last 6 months
- – 40% at least once a month
- – 58% hug or kiss at least once a week
- – 44% sexual touching / caressing at least once a week (64% if have a partner).
- – 22% masturbate at least once a week (25% of those with partners)
- – 43% were satisfied with their sex lives, this decreased with age.
Other key factors that affect sexual satisfaction include health (including medications), stress, financial situation and lifestyle practices such as exercise.
TILDA (Irish Longitudinal Study of Ageing) survey 8000 adults over 50.
- – 59% sexually active, of those 69% at least once a week or month
Sexual Desire in Later Life. DeLamater and Sill, Journal of Sex Research 2005
Reasons that sexual desire is reduced can be broken down into 3 main themes, although the most influential, was unsurprisingly, that attitudes towards sex were more important than biomedical factors.
- Biological reasons:
- More below
- Psychological reasons:
- – Sexual information
- – Attitudes towards sexual expression
- – Mental health conditions
- – Depressions/Treatment
Youth oriented culture therefore there is poor representation of sexual attitudes and expression with older adults. This includes media and advertising campaigns. Beauty products aimed at firmer, smoother, younger looking glowing skin etc.
Mastectomy; this surgery may cause some women to lose their sexual interest or their sense of being desired or feeling feminine. Similar with stomas.
- Social influences:
- – Availability of a partner
- – Length of relationship
- – Quality of relationship
Satisfaction within a relationship is deemed an important correlation with desire. Many older couples find greater satisfaction in their sex life than they did when they were younger. They have fewer distractions, more time and privacy, no worries about getting pregnant and greater intimacy with a lifelong partner.
Biological Factors:
Hormones
Both men and women’s sexual desire is driven by hormones.
- – Men: androgens, such as testosterone,
- – Women:oestrogen and androgens, again testosterone too
As women age there is a drop in both androgens and oestrogen by around 50% at the time of the menopause. A reduction in these hormones causes atrophic changes within the vagina diminishing vaginal lubrication which causes dryness leading to pain and/or discomfort. Painful sex maybe a contributing factor in reducing sexual activity. In ELSA 2012, 30% of women aged 70-79 reported vaginal dryness and 15% reported vaginal pain. Between 30-40% women in all age brackets over 60 reported usually, or always having difficulty with arousal or orgasm.
Lack of lubrication also makes abrasions and tears in the vaginal wall more likely leading to increased risk of transmission of infections. Also increases risk of recurrent UTIs and symptoms can be similar.
The pain/discomfort itself might not reduce the desire to have sex however the 50% reduction in the driving hormones might reduce sexual desire.
For men the decline in testosterone is slightly slower paced and from the age of 40-70 years the drop is about 30%. Prolonged time to erection. 30% men reported some degree of erectile dysfunction (AARP) i.e. never or only sometimes able to get and keep an erection sufficient for sexual intercourse. In ELSA study, this was seen most frequently in the over 80s group (50-70%).
Prostatectomy; Can be both curative for cancer or treatment plan for those with an enlarged prostate. It may cause urinary incontinence or erectile dysfunction, (a statistic here would be helpful). There are some medications and devices that might reduce the frequency of erectile dysfunction.
How long will I love you?- Sex and intimacy in later life. ILCUK February 2017
Chronic diseases
CVD, diabetes, arthritis and cancer all negatively affect sexual desire both directly acting on physiological mechanisms, vascular processes, and reproductive structures, limiting body function.
Lots of studies talk about the decline in sexual desire post MI and stroke but the literature doesn’t compare pre illness and post illness desire. Those with CVD, HTN, PVD statistically have a lower sexual desire and are also more likely to have MI’s & strokes.
It is proven that men with diabetes have lower sexual desire compared with those of the same age without diabetes. The duration of the diagnosis i.e since childhood, or the type, type 1/type 2, the medication (insulin/non-insulin) wasn’t considered in the findings.
Women with diabetes have been studied considerably less. One study suggested that diabetic neuropathy might affect the nerve supply to the pelvis in women but the evidence is a bit sketchy. Women with diabetes are proven to experience a higher than average rate of yeast infections, and although easily treatable, may reduce sexual desire.
Continence
Incontinence is more common as we age, especially in women. Extra pressure on the belly during sex can cause loss of urine, which may result in some people avoiding sex. This can be helped by a change in positions. The good news is that incontinence can usually be managed to prevent this from happening.
Conditions of circumstances that may impact or limit this
Reduced Mobility
Joint pain due to arthritis can make sexual contact uncomfortable. Exercise, drugs, and possibly joint replacement surgery may relieve this pain. Rest, warm baths, and changing the position or timing of sexual activity can be helpful, within 4 hours of analgesia. Arthritis research UK has provided a helpful booklet with different positions in to try depending on what might be painful.
http://www.arthritisresearchuk.org/arthritis-information/daily-life/sex-and-arthritis.aspx
The article isn’t specifically related to older people but mentioned that sexual ability was important to 58% of the sample and ageing had a negative impact on its importance (P<0.005). Data relates specifically to RA only.
Those with catheters talked about how their catheter and their disability affected their sexual self-esteem, feelings of masculinity or femininity, and how the catheter cause pain, discomfort, or unexpected symptoms during sex. Many noted the lack of information on the subject and also said that health professionals were reluctant to talk about sex.
Medications:
Antidepressants and antihypertensives medications are known to affect sexual function. Alpha-blockers, diuretics and calcium 2 channel blockers all known to prevent sexual function in men. Lots of theories why this might be the case in women but no rigorously tested outcome as yet.
Psychiatric medication decreases sexual desire. SSRI’s is a major culprit for this as the side effects are known to reduce sexual desire, cause erectile dysfunction, and increases the difficulty in achieving orgasm both through sex and masturbation.
SSRI is first line treatment for elderly population as the least cholinergic side effects and interactions. Generally thought of as equally as effective in anxiety and depression as CBT however the uptake of CBT is less.
The good thing is that SSRI sexual dysfunction is very much dose dependent. So those on very low doses might not experience the side effects listed above. It could be important to establish the importance of sexual desire/function of the individual prior to commencing SSRIs.
There are those drugs that increase libido. Dopamine agonists, (example), cause impulse control disorders so hyper sexuality is a common problem with them and there have been a lot of case studies done on the effects of this. Some case studies identified increased sex drive which was thought to be medication related.
Prostate Problems
Men with prostate disease have measurable less sexual desire; however sexual dysfunction is a common complication of prostate disease which is likely to be the cause of the reduction in sexual desire -> cycle.
Specific considerations to the current older generation
Sexually Transmitted diseases:
In 2008, the prevalence of those diagnosed with HIV/Aids flipped from being younger adults to those 45 and over. The highest rates of current diagnosis are those over 54. Limited research on those diagnosed with STIs over 55.
A generation who now don’t need to worry about pregnancy and never had sex education so therefore may not know about STI’s and HIV/Aids transmission may not deem themselves as having risky sex.
Condom use is less common in older adults, including those not in monogamous relationships. In those defining themselves as single and dating 50% of men and 29% women reported using a condom rarely or not at all. (Fisher et al, 2010)
Dementia
Relationships
Some people with dementia show increased interest in sex and physical closeness as inhibitions decrease and in frontotemporal dementias especially. Those with severe dementia may not recognize their partner but still seek sexual contact or be attracted elsewhere. In later stages, role as carer and partner may be conflicting, or potentially comforting
Consent
This could be a potentially tricky area with high risk for vulnerability and need for safeguarding but we need to ensure we aren’t overly paternalistic.
Legalities
– Case law appears to recognise that decisions in relation to sexual activity are more ‘visceral’ that ‘cerebral’ and therefore whilst the ability to use and weigh up information is important it is unlikely to loom large than in other assessments of capacity.
- – In other differences from usual MCA process, when someone lacks capacity, another person cannot consent on their behalf, unlike all other aspects of best interests decision making.
- – MCA does not allow for people to make advance decision in relation to sexual matters.
Assessing capacity
To assess capacity case law considers whether the person understands a number of general issues:
- – the mechanism of sex;
- – the risk of sexually transmitted diseases (and pregnancy in younger people); and
- – they understand they can refuse – a person doesn’t need to understand all three.
Also important to assess whether the person with dementia recognises the person they are having the relationship with; whether they can express their views and wishes within the relationship, or how they will be affected by rejection. Important that sex is mutually pleasurable and not meant to hurt or degrade.
The Sexual Offences Act (2003), which makes it a criminal offence to deliberately target vulnerable people for sexual gain. A vulnerable person may be exploited even where they are apparently consenting to sexual activity if they do not recognise if they are being mistreated or manipulated. Where there are differences in cognitive abilities between two people, there is a potential for abuse due to the unequal power dynamic.
If the person is deemed to lack capacity this would lead to a level of supervision that would prevent the person engaging in sexual activity, which potential amounts to a DOLs.
This probably explains a lot of our paternalistic attitude but it is just as important to facilitate well being. If this is not discussed then you will not be able to address it. There are several guides available to help you explore this further
Care Home Residents
While care home staff agreed that addressing sexual issues should be part of holistic care and there being evidence that residents would welcome such discussions, it is often not addressed. Assumption of heterosexuality is usually the norm in care home settings.
Sexuality in Older Adults: Effect of an education intervention on attitudes and beliefs of residential aged care staff. Bauer et. al 2012
The Final Taboo is an guide for those working with dementia in a care home setting, covers how to assess needs and provide support. Covers some questions around capacity, wider ethical considerations as well as practical framework for assessing sexual expression in a non-judgemental and supportive way. Also provides links to relevant policy and studies in this area.
- 1) What form does the behaviour take?
- – In what context?
- – How frequently does it take place?
- – Review the resident’s behavioural history and current routine.
- 2) Consider speaking to the resident’s family, friends or partner to gain a greater understanding of their social and sexual history.
- – What factors may contribute to this? Could there be a social, environmental, medical or psychological cause?
- -Has there been a change to the resident’s routine or environment? For example, sometimes a lack of privacy can force patients to express sexual behaviour in an overt fashion (Manchip et al, 2007).
- – Is it possible that the resident is misinterpreting the actions of, for example, the care worker or believes them to be someone else they know well or intimately?
- – Have you checked the resident has no underlying medical condition which may be contributing to this behaviour?
– Or that their medication has been changed? For example, urinary or vulva/vaginal problems may lead to increased touching.
- – Have you assessed the resident’s mental wellbeing? – – — Could they be depressed, manic or simply feeling lonely and looking for reassurance, comfort or touch?
- – If the resident is trying to take their clothes off, is it because they are wearing an item of clothing that is irritating them?
- 3) Reflect on how you define and classify inappropriate behaviour
- – Consider how you have formed this judgement and try to work out if the behaviour offends your attitudes, cultural
beliefs or values. Or do you find the behaviour inappropriate because you feel it would be judged so by other staff
members, residents or maybe the residents family?
- 4) Consider what risks are involved
- – Does the resident pose a risk to other residents? A risk to themselves? Or to the wider residential community?
- – Try to assess the awareness and understanding the resident has of their behaviour.
- – Continue ongoing assessment of the resident’s mental capacity.
-
5) Looking after yourself
- – It is understandable that you may feel upset and/or angry and/or emotional if you have been subject to aggressive or inappropriate behaviour.
- – Seek support and reassurance from your colleagues.
- Make sure you report and record any behaviour that may be inappropriate.
The Final Taboo– A guide to dementia, sexuality, intimacy and sexual behaviour
Bringing it up
The biggest problem with older adults and sex is talking about it and limited conversations that healthcare professionals have with patients/clients on this matter.
https://www.alzheimers.org.uk/download/downloads/id/1801/factsheet_sex_and_intimate_relationships.pdf
Curriculum Mapping:
Curriculum
NHS Knowledge skills framework
Area
Suitable to support staff at the following levels:
- – Personal and People
- – Development: Levels 1-3
- – Service Improvement: Level 1 – 2
- – Equality and Diversity level 1
Foundation Curriculum 2016
- 2- Patient as centre of care
- 6- Communication with patients
- 10- Support for patients with long term conditions
Core Medical Training
The patient as central focus of care
Relationships with patients and communication within a consultation
GPVTS program
Section 2.03
The GP in the Wider Professional Environment
- – Core Competence: Managing medical complexity
Section 3.05 – Managing older adults
- – Core Competence: Managing medical complexity
- – Core Competence: Working with colleagues and in teams
- – Core Competence: Practising holistically and promoting health
- – Section 3.08 – Sexual Health
ANP (Draws from KSP)
Section 9&10 CGA
Section 20&21 Patient as central focus of care
Section 29 Communication
Section 36 Psychological, social, cultural, ethnic and economic factors